
Genesis of Atherosclerosis
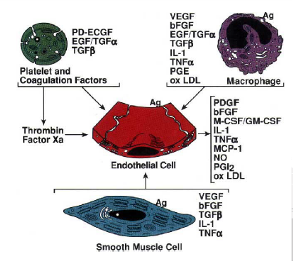
Figure 1 – Genesis of Atherosclerosis
Early on atherosclerotic lesions start as ‘fatty streak’, which is an extracellular lipid pool with an accumulation of lipid-rich macrophages and T lymphocytes within the inner surface of the artery wall (intima).1,2 These fatty streaks develop into layers of smooth muscle cells and lipid-laden macrophages, entering the intermediate lesions (preatheromatous lesions) stage. This stage is known as pathologic intimal thickening (PIT).2,4 Later on these preatheromatus lesions evolve into more complicated, occlusive lesions known as fibrous plaques. These fibrous plaques enlarge in size and eventually project into the lumen of the artery wall, disrupting the blood flow.2 According to Russell Ross, in the genesis of atherosclerotic lesions, the endothelium interacts with macrophages, platelets, smooth muscle cells and T lymphocytes. Each of the stages in the lesion progression is reversible. Figure 1 depicts the genesis of plaque and figure 2 shows the macrophages in atherosclerosis.

Figure 2 – Macrophages in Atherosclerosis
ASVD leads to different categories of cardiovascular diseases (CVD) depending on the location and nature of the blocked artery. Atherosclerosis leads to coronary heart diseases (CHD) when atherosclerotic plaques build up in the arteries in the heart. Coronary heart diseases lead to chest pain (angina) and heart attack (MI) when the blood supply to the heart is restricted. When atherosclerosis occurs in the arteries that provide blood supply to the brain, it can lead to stroke, eye stroke (blindness), numbness, impaired speech, vision, balance and coordination. Peripheral artery diseases (PAD) happen when the plaque builds up in the arteries of arms and legs restricting the body supply to these body parts. The common warning signs for this condition are leg or hand pain on exertion, increased sensitivity to heat and numbness in hand or leg. If untreated, this could lead to gangrene and amputation. If atherosclerotic lesions develop in the arteries that feed the kidneys and cause blockage of blood supply to this vital organ, it can lead to kidney failure, high blood pressure and sometimes to renal artery stenosis.,/br>

Figure 3 – Development of Atherosclerosis
Plaque rupture is more common in symptomatic than asymptomatic patients as the fibrous plaque cap of symptomatic patients is thinner with greater inflammatory infiltrate. There are certain risk factors such as high blood pressure ( hypertension), high blood cholesterol (hypercholesterolemia), low HDL-cholesterol and the ratio of total to HDL-C that places asymptomatic patients (carriers of disease with no symptoms) at an increased risk level for carotid plaque rupture and thrombosis. Hence it is imperative that we identify these high risk patients for acute major cerebrovascular accidents early on using non-invasive imaging diagnostic techniques to locate and evaluate the progression of stable non-flow limiting plaques and decide the treatment options available for these individuals.
Arteries are vessels that carry blood and oxygen from the heart to the entire body and they contain three layers of cells. The interior surfaces of arteries (tunica intima or lumen) are lined with a monolayer of flat epithelial cells called endothelium. The endothelium regulates the tone of arteries thus aiding in smooth blood flow. The middle layer (tunica media) is made of smooth muscle cells (SMC) entrenched in a complex extracellular matrix. The adventitia, the outer layer of arteries, contains mast cells, nerve endings and microvessels.3 We can see in Figure 3 the developmental process of atherosclerosis and how the hardening of the walls can slowly block the blood flow of the arteries.
Stage 1 [Foam cells formation] The risk factors that could start or trigger ASVD damage the endothelium. Bad cholesterol or low-density lipoprotein (LDL) passes through the damaged endothelium into the artery wall.The LDL molecules inside the artery are prone to oxidation by free radicals and become toxic to the cells. The body’s immune system responds by streaming in white blood cells (monocytes) to absorb the toxic oxidized-LDL molecules in the damaged artery wall. Monocytes are divided into macrophages to ingest the oxidized LDL molecules leading to the formation of foam cells.

Figure 4.1 – Cross Sectional representation of atherosclerotic lesion progression
Stage 2 [Plaque formation] Foam cells attach to the intimal smooth muscle cells of the artery and grow within it. In this stage smooth muscle cells (SMC) from the middle layer of the artery wall (media) migrate into the inner layer (intima), the SMCs present in the intima and the migrated SMCs from media propogate, and the additional synthesis of extracellular matrix macromolecules such as collagen, elastin and proteoglycans leads to the progression of lesions in the artery wall.3 These foam cells signal the immune system to release cytokines, which leads to the release of more white blood cells and the whole cycle starts again. This cycle repeates many times util the artery wall becomes inflamed and atherosclerotic lesions are formed. This accumulation of LDL molecules, cholesterol crystals, microvessels, foam cells, fat, cellular waste, calcium, platelets and fibrin becomes plaque (atherosclerotic lesions) in the inner lining of the artery wall. Extracellular lipids from dead and dying foam cell macrophages build up in the central region of a plaque, known as the lipid or necrotic core.3 In response to plaque buildup, the artery cells are simulated to produce additional substances and form a hard cover (fibrous cap of connective tissue) over the damaged section separting the plaque from the lumen. This leads to narrowing of arteries, reduction in blood flow and oxygen to the body and increase in blood pressure. In case of moderate artery narrowings, the blood flow is restricted on excertion leading to pain and pressure in different body parts.
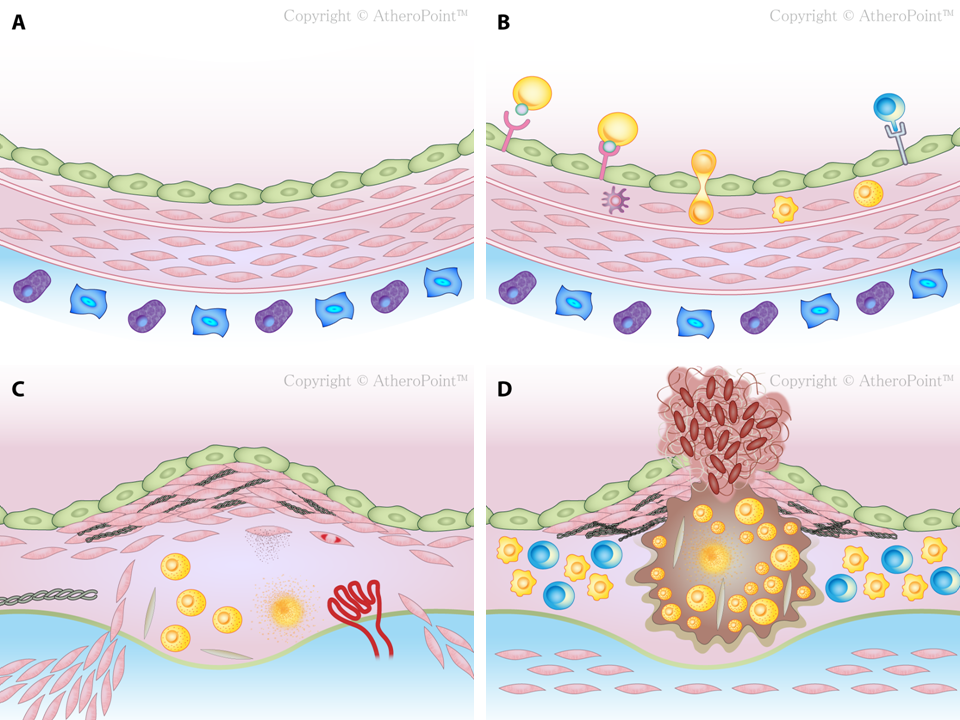
Figure 4.2 – Detailed pictorial representation of atherosclerotic lesion progression
Stage 3 [Thrombus formation] Overtime macrophages release certain enzymes to degrade the hard cover, leading to plaque rupture. Plaque rupture triggers the platelets, causing the blood to clot inside an artery at the site of atherosclerotic lesions. There are more macrophages in the margins of the fibrous cap of the plaque, hence a rupture in these margins leads to bleeding into the plaque and eventual thrombus in the blood vessel by the platelets. These blood clots can either partially or completely block an artery, thus reducing the oxygen supply to crucial body organs. A clot in the carotid artery leads to stroke in the brain and a clot in the coronary heart leads to heart attack. Blockage of an artery in the kidneys can lead to kidney failure and a block in the arteries of thighs and arms could result in gangrene and amputation. Figures 4.1, 4.2 and 5 show in detail the progression of atherosclerosis through all the stages discussed above.
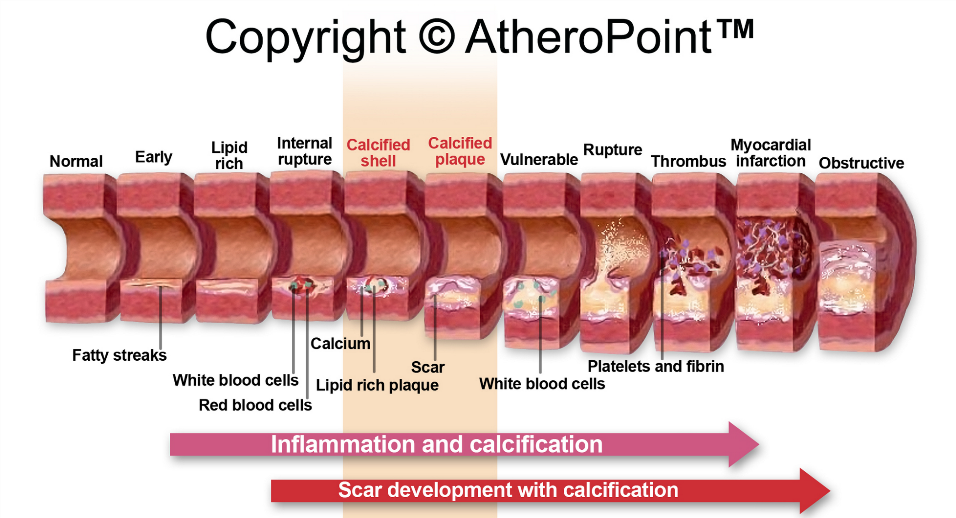
Figure 5 – Stages of progression in atherosclerosis