
Diabetes and Atherosclerosis
Statistics on Diabetes
According to the data from 2011 National Diabetes Fact Sheet 8.3% (25.8 Million) of Americans have diabetes and an estimated 79 million adults have pre-diabetes, a state in which blood sugar levels are elevated than normal, but not high enough to be categorized as diabetes and this increases an individual’s risk of type 2 diabetes, heart disease and stroke.
Diabetes, the seventh leading cause of death, accounts for a total of 231,404 deaths in a year. The total estimated cost of diagnosed diabetes has increased from $174 billion in 2007 to $245 billion in 2012, a 41% rise in cost. Diabetes increases the risk of stroke by 2 to 4 times and the death rate related to heart disease by 2 to 4 times in comparison to an adult without diabetes.
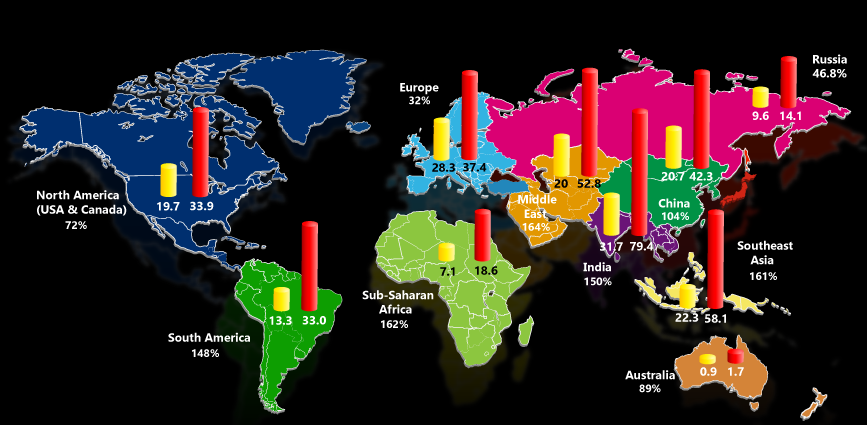
In 2011, 366 million people of the global population had diabetes, and this is projected to rise to 552 million by 2030. Diabetes accounted for 4.6 million deaths worldwide in 2011 and it caused $465 billion dollars in healthcare expenditures. Globally, diabetes is the eighth leading cause of death. The projected global change in diabetic population from 2000 to 2030 is captured in the map displayed below.
What is Diabetes?
Diabetes, also known as diabetes mellitus, is a metabolism disorder in which a person has high blood glucose, either because the body (pancreas) does not produce adequate insulin [Type 1 Diabetes], or because the body’s cells do not react properly to insulin that is produced and the cells become resilient to insulin action [Type 2 Diabetes], or both. The common symptoms for patients with high blood sugar are frequent urination, increased thirst and hunger. Diabetic patients may also experience sudden weight loss, fatigue, blurry vision, high blood pressure and high levels of ketones in urine.
Patients with type 1 diabetes are treated with insulin injections for the rest of their life. Type 2 Diabetes can be treated with medications and life style changes. Type 2 Diabetes can be controlled with weight loss, healthy diet, regular exercise and constant blood sugar monitoring.
If left untreated, diabetes can lead to several acute and long-term complications such as diabetic ketoacidosis, diabetic coma, cardiovascular disease, diabetic retinopathy, hearing loss, diabetic neuropathy, ulcers, gangrene, nephropathy, peripheral arterial disease and stroke.
Pathogenesis of Atherosclerosis in Diabetes Mellitus
The onset and progression of atherosclerosis is accelerated in patients diagnosed with diabetes mellitus. The interior surface of the arteries (tunica intima) has a lining called endothelium which is a monolayer of flat epithelial cells. This endothelium layer is the interface between blood and tissue that regulates the blood flow, delivery of the nutrients and coagulation and thrombosis formation. This endothelium produces Nitrous oxide (NO) while aiding in the smooth blood flow.They further produce prostaglandins and angiotensin II, that regulates the function and structure of the arteries. When the vessel wall dilates,the arteries relax, which means the regulation is happening well and there is no sticking of the cells to the vessel walls. The below two sections describe in detail the role played by diabetics in the developmental process of atherosclerosis in arteries.
Role of Insulin in Normal & Diabetic Patients
Insulin is produced by the pancreas which helps in production of NO by these epithelial cells of the blood vessel linings. It is this NO which prevents the leukocyte adhesion to the endothelium layer of the arteries. It is this NO, which slows down the inflammation. When the blood flows fast in the healthy artery, ERK-5 (extracellular signal-regulated kinase 5 ) enzyme is triggered which signals eNOS (nitric oxide synthase) and hence dilates the blood vessels. KRK-5 also triggers enzyme KLF2 (Kruppel-like factor 2) and PPARg (peroxisome proliferator-activated receptor-g) and this provides the capability of prevent the capability of cells to stick to the blood vessels.
In diabetics who are resistant to insulin, the stimulation of NO by insulin is lost, this increases the tendency of more plaque formation in the blood vessels. This triggers adverse events of the metabolic activity within the endothelial cells of the arterial wall. The elevated levels of blood glucose and resistance to insulin in diabetic patients also increase the production of substances that narrow and harden the blood vessels. High blood glucose increases the production of highly reactive molecules known as free radicals. Thus diabetes worsens Atherosclerosis disease formation. Figure 1 depicts in detail the pathophysiology of the blood vessel in diabetic pateints.
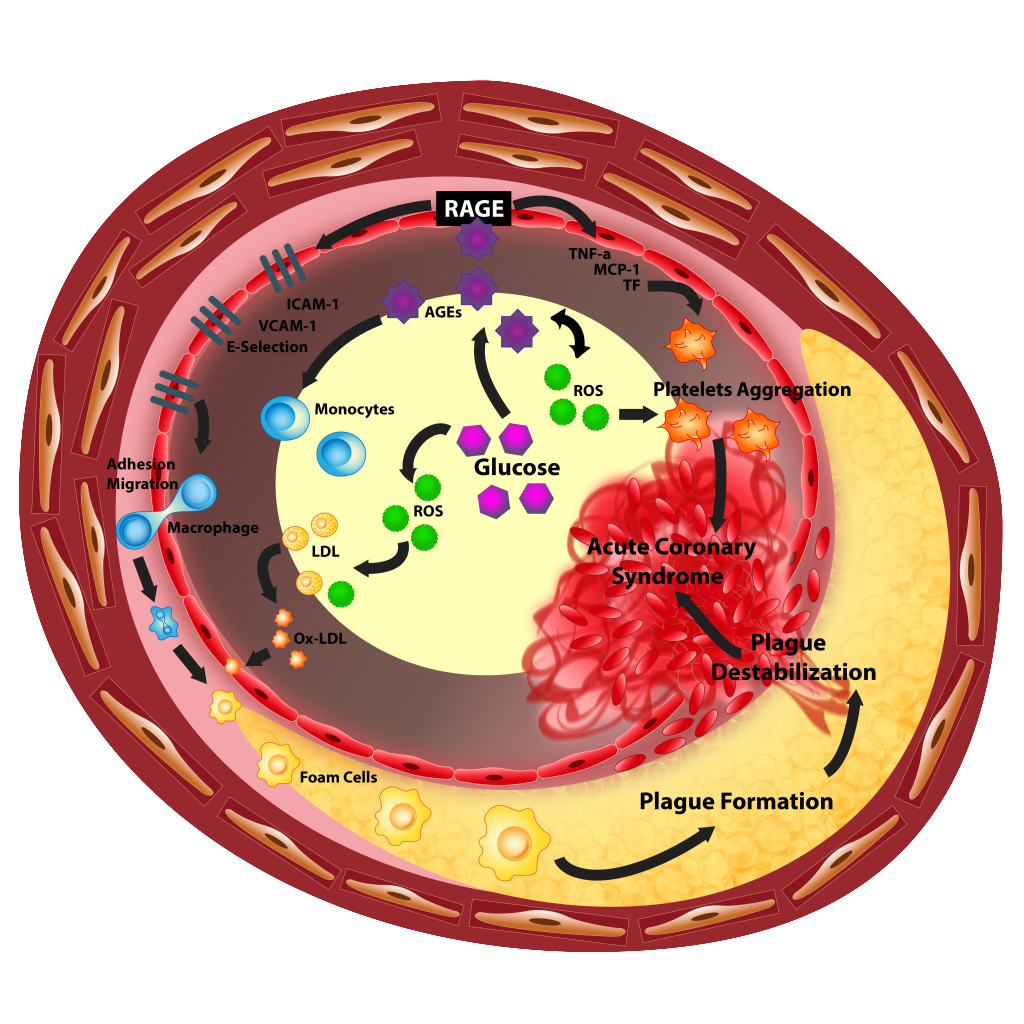
Figure 1 – Pathogenesis of Atherosclerosis in Diabetes
Collagen breakdown in diabetic patients leading to stroke
Collagen provides the stability to the fibrous cap of the plaque in the blood vessels. In Diabetic patients, there is a production of metalloproteinases, which leads to breakdown of collagen. When collagen breaks down, plaques rupture and trigger the formation of thrombosis. This leads to vascular occlusions.
Link between Diabetes and Atherosclerosis
There is a strong link between diabetes and atherosclerosis disease. When the blood sugar level rises, free radicals like fatty acids and triglycerides rise. As a result, cell components like DNA tears apart causing cell death or apoptosis. Due to death of the cell, the nitric oxide content in the cell decreases. The vessel walls become stickier due to the high blood sugar. The dead cells start to stick to the walls and reduce the blood flow. The enzyme ERK5, KLF2 and PPAGg decreases and there is a reduction in blood relaxation and worsening the plaque formation or lipid formation by sucking the dead cells in the pathway. This causes the vessel wall to block the blood flow further. In diabetics who are resistant to insulin, the stimulation of NO by insulin is lost, this increases the tendency of more plaque formation in the blood vessels. The elevated levels of blood glucose and resistance to insulin in diabetic patients also increase the production of substances that narrow and harden the blood vessels. High blood glucose increases the production of highly reactive molecules known as free radicals. Thus diabetes worsens Atherosclerosis disease formation.
As a result, Endocrinologists would be very interested in measuring the carotid IMT/IMTV if they are using ultrasound for their screening. Recently there have been many clinical papers relating HbA1c, which is an indicator of blood glucose levels and IMT measurements. This is very important for Diabetic patients.
Diabetes, Atherosclerosis and AtheroEdge
Intima media thickness of the carotid arteries (cIMT) is a validated surrogate marker of early atherosclerosis and is associated with coronary atherosclerosis and with the risk of future vascular events. Because it can be measured relatively simply and noninvasively, it is well suited for use in large-scale population studies. Ultrasonic measurements correlate well with histology and increased IMT is associated with vascular risk factors and the presence of more advanced atherosclerosis, which includes coronary artery disease (CAD). In the past years, the cIMT was calculated by the sonographers that performed the examination by tracing a line between the two interfaces lumen\intima and media\adventia. In the last years, thanks to the rapidly growing hardware and algorithms analysis, it has became possible to automatically calculate the cIMT avoiding one of the most important limits of the manual analysis of the IMT: the poor inter\intra-observer agreement.
The important role of long-term hyperglycemia in the development of atherosclerosis is known and a correlation between HbA1c and cIMT was demonstrated especially in women and in children affected by type 1 diabetes. The accurate monitoring in critical patients, such as the patients with type 2 diabetes, is crucial since persons with diabetes have 2-6 folds higher cardiovascular risk than subjects without diabetes. Recently, male gender has also been associated to a more rapid increase of the cIMT in Type 2 diabetes, thus further increasing the need for accurate measurement and monitoring. In a recent review, Kurukulasuriya and Sowers showed that the reduction of the glycated hemoglobin (HbA1c) is associated with a lower incidence of myocardial infarction, but they also evidenced that the management of the cardiovascular risk factors experienced by patients with type 2 diabetes required a multidisciplinary approach with implementation of strategies to improve the underlying cardiovascular risk factors. It is, therefore, evident that accurate diagnostic and prognostic vascular tools are needed in association to the study and assessment of patients’ HbA1c levels.
Carotid IMT is considered a reliable measure of generalized atherosclerosis. Previous investigation have demonstrated that a thickened cIMT is correlated with an increased risk of stroke and myocardial infarction and it is predictive of future events of coronary heart diseases in subjects with type 2 diabetes.[1][2] In a recently published study by Herder et al. [3] in a population of 2741 patients, it was found that the diabetes was predictor for IMT and IMT progression, whereas the total cholesterol, smoking, and systolic blood pressure were stronger long-term predictors of carotid plaque area and carotid plaque area progression than for IMT and IMT progression.
Research has shown that the cIMT identified by using automated software called AtheroEdge™, which can process a large set of ultrasound images automatically, was associated with HbA1c levels in a population affected by coronary artery disease. Recently, a study was purposed to evaluate whether the cIMT, identified by using AtheroEdge™ automated software, is associated with HbA1c in Coronary Artery Disease Patients and the study found a strong association between cIMT, measured by the means of AtheroEdge, and HbA1c in the whole study population (p = 0.0007).
Our methodology of automated cIMT measurement using AtheroEdge has demonstrated an excellent reproducibility and accuracy. Therefore the association we found between the cIMT and HbA1c can be considered further strengthened by the methodology for the IMT quantification.
References
- Bernard S, Serusclat A, Targe F, et al. Incremental predictive value of carotid ultrasonography in the assessment of coronary risk in a cohort of asymptomatic type 2 diabetic subjects. Diabetes Care 2005; 28: 1158-62.
- Yamasaki Y, Kodama M, Nishizawa H, et al. Carotid intima-media thickness in Japanese type 2 diabetic subjects: predictors of progression and relationship with incident coronary heart disease. Diabetes Care 2000; 23: 1310-5.
- Herder M, Johnsen SH, Arntzen KA, Mathiesen EB. Risk factors for progression of carotid intima-media thickness and total plaque area: a 13-year follow-up study: the Tromso Study. Stroke 2012; 43: 1818-23.